Biopsy Definition
A biopsy is the removal of tissue or cell samples for the purpose of examination using various biological techniques to gain information regarding the disease status of a particular tissue. Biopsies are typically conducted by surgeons or other interventional specialists (e.g., radiologists or cardiologists). The biopsied tissue sample can be stained and microscopically examined by experts who determine if there are any histological abnormalities or score the sample to evaluate the extent of disease (see the image below for an example of a histological sample obtained from a biopsy).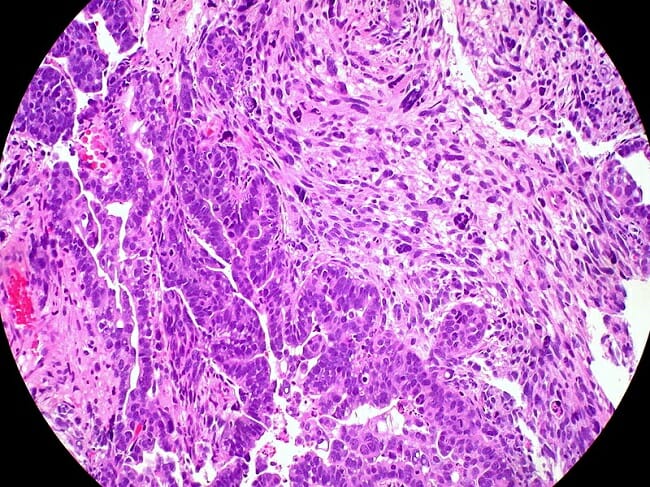
Biopsies can also be enzymatically digested and assessed by various molecular techniques (e.g., polymerase chain reaction [PCR], Western blotting, enzyme-linked immunosorbent assay [ELISA]), and multi-color flow cytometry to identify the expression of pathological biomarkers or proteins. The most common purpose of a medical biopsy is to identify the presence, stage, and specific diagnosis of a type of cancer or other diseases. There are three distinct types of biopsies: incisional, excisional, and needle aspiration biopsies.
Types of Biopsy
Incisional Biopsy
An incisional biopsy is also referred to as a “core biopsy” and involves the extraction of a tissue sample for laboratory analysis. When collecting incisional biopsies, the histological integrity of the tissue is preserved. This ensures that the examining pathologist can perform a thorough histological analysis of the sample, for the identification of any specific cellular changes or protein expression. In such samples, the distribution of cells and any characteristic histological changes within the tissue can also be visualized. For example, in patients with cirrhosis of the liver, a tissue pathologist will assess an incisional biopsy for hepatocellular dysfunction, fibrosis, and the presence of inflammatory cells distributed throughout the sample of liver tissue. Incisional biopsies are often collected with an instrument that takes a “bite” out of the tissue that is being investigated. The histological section below is an example of a biopsy specimen obtained from a core biopsy.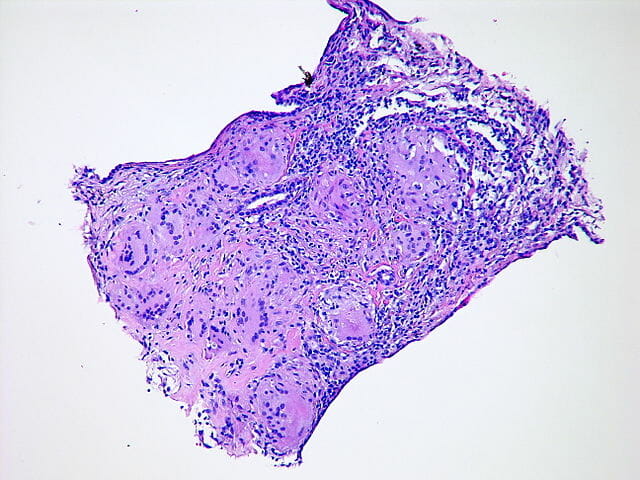
Excisional Biopsy
An excisional biopsy involves the extraction of a diseased tissue or lump. The most common forms of excisional biopsies involve the removal of suspicious moles or lumps under the skin, as well as entire tumors. Typically, suspicious lumps residing under the skin are small and easily biopsied. The pathologist will have the tissue samples sectioned, stained, and microscopically reviewed in order to diagnose the lesions. The most common purpose of an excisional biopsy is to detect the presence and type of cancer. Large excisional specimens from cancer patients are termed “resections”. The example below is an excisional biopsy from a lumpectomy performed on a patient with breast cancer.
Needle Aspiration Biopsy
A needle aspiration biopsy involves collecting a tissue or fluid sample using a large bore or fine needle (as seen below), depending on the specific requirements. In contrast to incisional biopsies, a needle aspiration biopsy only extracts a small fluid sample or cells from a particular region. As such, the entire histological picture of the diseased region cannot be analyzed. Needle aspiration biopsies are typically tested for the presence of inflammatory mediators (e.g., cytokines), abnormal protein signatures (e.g., cellular biomarkers), and morphological abnormalities of the local cells (e.g., cancerous versus non-cancerous cells).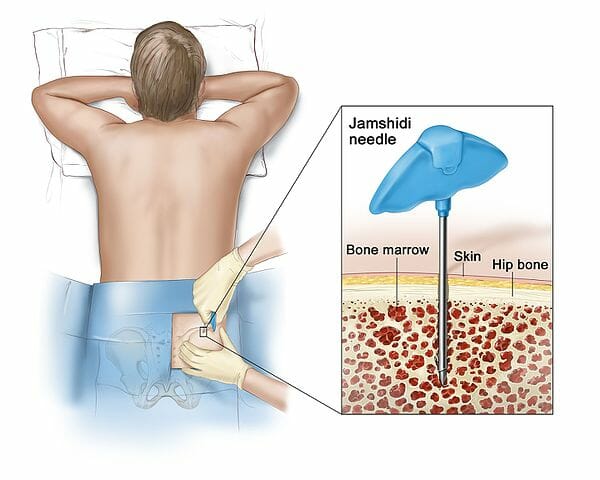
Cancer Biopsies
A wide range of methods are used for perform biopsies when a cancerous lesion is identified or suspected. If possible, surgeons will perform an excisional biopsy to extract the entire tumor. The pathologist analyzing the tissue will determine the diagnosis, as well as examine the surgical margin of the tumor biopsy to assess whether the diseased tissue extends further than that biopsied. Depending on whether cancer is identified at the biopsy margins, further excision may be required. Biopsy margins are deemed “negative” if the margins are clear of any disease, and “positive” if cancerous cells are identified at the margins. Such biopsy specimens are typically histopathologically graded to determine the stage of cancer progression, in addition to the specific type of cancer.
Under circumstances in which an excisional biopsy is not possible, a portion of the tissue is collected as an incisional or needle aspiration biopsy. It is common for these types of biopsies to be performed prior to an excisional biopsy to establish the specific diagnosis, as well as classify a suspicious lesion as malignant (cancerous) or benign (non-cancerous). Such suspicious lesions are usually identified via a variety of imaging techniques (e.g., computed tomography [CT], magnetic resonance imaging [MRI], ultrasound, and X-ray). For example, an X-ray of a patient’s lungs may reveal a suspicious lesion, for which a needle or core biopsy would typically be performed to diagnose the lesion before attempting a full extraction. Often, following diagnosis using a needle biopsy, the patient will undergo chemotherapy to shrink the tumor prior to performing a complete resection.
Biopsies for Inflammatory Diseases
While lesions suspected to be cancerous are the most common biopsy samples, biopsies will also be collected for the diagnosis of various inflammatory diseases. Such diseases that often require a biopsy include vasculitis (biopsy of the arteries), kidney disease, infections (biopsy of swollen regions, including lymph nodes), transplant rejection (biopsy of the transplanted organ), rheumatoid arthritis, and intestinal diseases (biopsy of the intestine; the region differs depending on the location of inflammation [e.g., ulcerative colitis versus Crohn’s disease]). Depending on the disease and location, the specimen will be tested for functionality, protein expression, or histological appearance of the tissue. In cases of an infection, specific staining will be performed to visualize the presence of pathogens (e.g., Gram or Ziehl Neelsen staining for bacteria), PCR can be conducted to confirm viral infections, or a bacterial culture may be conducted to obtain a positive diagnosis.
Common Biopsy Sites
Since diseases affect different regions of the body, biopsies are collected from common locations due to the ease of obtaining the sample, location of the pathology, or limitations of tissue access (e.g., if deep access to the affected tissue is not possible). The following are common locations for the collection of biopsies:
- Liver (e.g., cirrhosis and fibrosis)
- Breasts (e.g., breast cancer)
- Gastrointestinal tract (e.g., ulcerative colitis and Crohn’s disease)
- Pancreas (e.g., pancreatic cancer)
- Bone marrow (e.g., blood abnormalities and cancers)
- Lungs (e.g., infections, cancer, fibrotic disease, etc.)
- Prostate (e.g., prostate cancer)
- Nervous System (e.g., central nervous system, nerves, and meninges)
- Lymph nodes (e.g., cancer and infections)
- Muscles (e.g., neuromuscular diseases)
- Urogenital system (e.g., bladder, renal, cervical, etc.)
Quiz
1. The following is NOT a procedure that can be performed for a sample obtained from a needle biopsy:
A. Flow cytometry
B. Protein analysis for the expression of biomarkers
C. Histological analysis
D. Cytokine analysis of the collected fluid via an ELISA
2. A patient presents with a suspicious mole. What is the most appropriate type of biopsy to use?
A. Incisional biopsy
B. Excisional biopsy
C. Needle biopsy
D. Core biopsy
3. A mammogram of a female patient reveals a lump deep within the breast tissue. What is the most appropriate biopsy to perform initially to determine whether it is cancerous.
A. Incisional biopsy
B. Excisional biopsy
C. Needle biopsy
D. Core biopsy
References
- Bruening W, Fontanarosa J, Tipton K, Treadwell JR, Launders J, and Schoelles K. (2010). Systematic review: comparative effectiveness of core-needle and open surgical biopsy to diagnose breast lesions. Ann Intern Med. 16;152(4):238-46.
- Jain A, Khalid M, Qureshi MM, Georgian-Smith D, Kaplan JA, Buch K, Grinstaff MW, Hirsch AE, Hines NL, Anderson SW, Gallagher KM, Bates DDB, and Bloch BN. (2017). Stereotactic core needle breast biopsy marker migration: An analysis of factors contributing to immediate marker migration. Eur Radiol. May 19. doi: 10.1007/s00330-017-4851-7. [Epub ahead of print].
- Odze R. (2003). Diagnostic problems and advances in inflammatory bowel disease. Mod Pathol. 16(4):347-58.
- Phelps RG and Lebwohl MG. (2014). Biopsy Techniques: Shave, Punch, or Excision? JAMA Dermatol.150(1):12-13.
- Puri A, Shingade VU, Agarwal MG, Anchan C, Juvekar S, Desai S, and Jambhekar NA. (2006). CT-guided percutaneous core needle biopsy in deep seated musculoskeletal lesions: a prospective study of 128 cases. Skeletal Radiol. 35(3): 138-43.
- Rougraff B, Aboulafia A, Biermann JS, and Healey J. (2009). Biopsy of Soft Tissue Masses: Evidence-based Medicine for the Musculoskeletal Tumor Society. Clin Orthrop Relat Res. 467(11): 2783–2791.
Biopsy
No comments:
Post a Comment